Our Outcomes: Specialized Treatment for Survivors of TBI
What is known today as NeuroRestorative originally began in 1977 in Carbondale, IL, as the first-ever after-hospital specialized community-based residential brain injury rehabilitation program. Now providing quality programs supporting adults, children, and Veterans across 28 states, NeuroRestorative has grown to serve the unique needs of each person recovering from brain injury or Neurotrauma. Our quality outcomes have led to our programs’ growth in an ever-increasing number of locations, each providing an environment of care that maximizes opportunities for abilities and skill development, adjustment to disability, and community participation.
Families, funders, and all stakeholders care deeply about the features and benefits that NeuroRestorative programs provide. Still, it is the measurable difference we make in people’s recovery – the gains they achieve from the time of admission to the time of discharge, that cement the value of our programs. NeuroRestorative is proud to be an industry leader in outcomes collection, organization, and reporting, ensuring that the research, advocacy, and education we provide are rooted in the science of our measurement systems. This is critical because each person’s outcome is our focus for each individual we serve. Call us today to learn more about how we can provide the tools to help you or your loved one.
Each year, approximately 2.8 million people in the US sustain a traumatic brain injury (TBI). A TBI disrupts performance in multiple areas, including mobility, communication, cognition (memory and information processing), and emotional/behavioral functioning. Our treatment programs address each area of potential impairment with highly skilled treatment teams that include supports and services provided by: Physicians, nurses, physical therapists, occupational therapists, speech pathologists, psychologists, counselors, life skill trainers and more. Following post-hospital rehabilitation treatment, over 80% achieve a meaningful reduction in disability, and most can return home and resume productive activities. The charts and graphs below present the demographics, chronicity, and outcomes for over 2000 persons who sustained a TBI and completed our neurorehabilitation programs.
TBI affect people of all ages. Age groups that have the highest rate of TBI include: Children aged 0-4, adolescents aged 15-19, and adults aged 65 and older. Males are more likely to experience TBI than females.
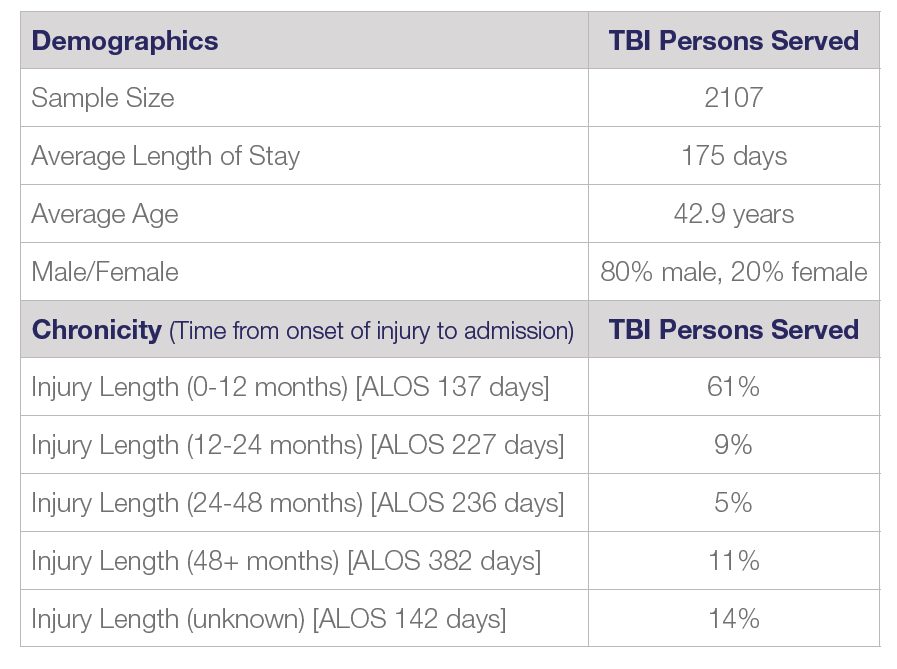
Chronicity Impact: Outcomes are significantly influenced by chronicity (Lewis, Horn & Russell, 2017). As such, when persons are able to access neurological rehabilitation care sooner, the individual has the highest chance of achieving successful outcome to rejoin their community and resume a productive lifestyle. If a person is admitted soon after injury, remediation strategies can be the focus of care. Lengthier time since injury slows the process of improvement and emphasizes greater use of compensatory strategy development with continuous skills reinforcement. For those admitted within one-year of injury, 58% were discharged home with a mild-moderate level of disability.
Residential vs. Non-Residential Care: The focus of residential services is to help progress a person from 24-hour assistive care to no longer needing constant supervision or assistance with daily living skills. The application of skills with community living becomes the focus of non-residential services.
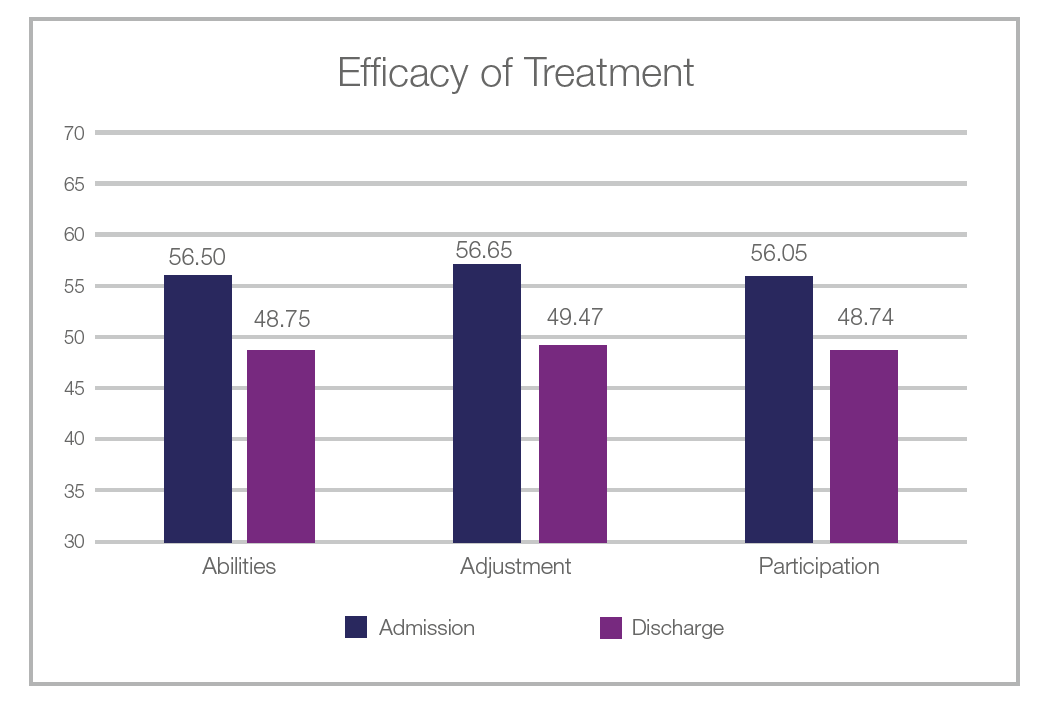
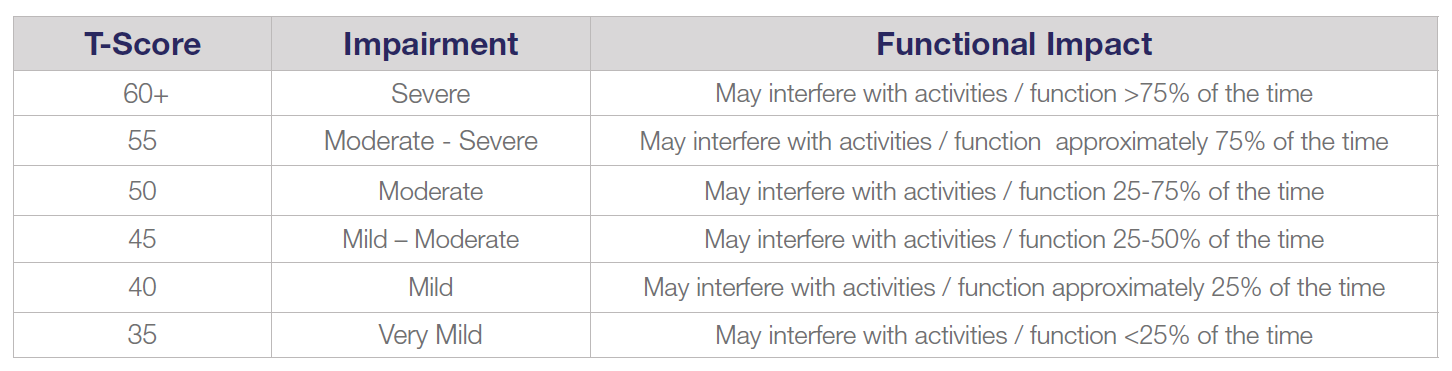
Outcomes are measured using the Mayo Portland Adaptability Inventory – Version 4 (Malec & Lezak, 2008). Lower scores indicate less disability. See the chart below for interpretation reference. The results provided in this graph demonstrate a significant and a meaningful change from admission to discharge with post-hospital care. This level of change is sufficient to reduce disability, leading to successful community discharge and societal participation.
Change Scores and Effect Size

The table above shows the change in score from admission to discharge. Change scores greater than 5 represent a clinically significant reduction in disability. Effect size measures the magnitude of change. An effect size of greater than 0.75 is considered to be a large and positive effect (e.g., reduction in disability). The vast majority of our TBI program graduates experienced this meaningful improvement in their functioning.
Mayo Portland Interpretation Guide